Miniaturization occurs in men and women who are balding. Miniaturization is the process where a normal thickness hair shaft becomes thinner and thinner over time due to the genetically determined effects of aging and/or androgenic hormones on the terminal (normal) hair follicle. The process of miniaturization is a slow process in genetic balding. Hair shafts may lose 10% of their diameter, then 20%, then 30% and so on. Each degree of increased miniaturization reflects further progression of the genetic balding process. The instruments that measure miniaturization were invented (and patented) by me in the early 1990s (patent ) and they are in wide spread use today. Socially detectable hair loss is not evident until more than 50% of average weight hair has been lost (more with fine, high contrast skin/scalp color hair and less with coarse, low contrast skin/scalp color hair) and as a result, many men do not seek out expert help until they see some evidence of balding (which they too often deny).
When a doctor views the scalp hair with high magnification, the degree of miniaturization and the location of the miniaturization are both critical to establishing (1) the diagnosis and (2) the rate of the process, which progresses over time. Because miniaturization is a relative measurement at any one time (comparing finer hair to the thickest hair), it takes substantial experience before this measurement can be useful to the individual clinician. In our experience, from examining and following tens of thousands of patients with the hair densitometer (video microscope), we have found that assessing the degree of miniaturization has useful predictive value when evaluating the risks of hair loss and in establishing hair loss patterns. The amount of miniaturization in each section of the scalp tells the physician just how far the balding is progressing or has progressed. In men who show more and more areas of miniaturization over time, the genetic balding can be considered active. In men treated with finasteride, if the miniaturization is reduced or the hair count is increased, it can be assumed that the balding process is coming under medical control.
We know that hair loss occurs in patterns (see Norwood Chart), but these patterns are what the eye can see. When the naked eye picks up these patterns, the miniaturization is always in a more advanced state. The balder the patient is, the worse is both the absolute hair count (density or healthy hairs) and the relative fullness of the miniaturized hair shafts. Clearly, miniaturized hairs that have a reduced hair circumference of 10% will have more bulk value than a hair circumference reduction of 70%.
In our practice we use a video densitometer to map each patient’s scalp. We typically map and digitally photograph a series of discrete areas on the scalp that reflect the balding and non-balding areas. The non-balding donor area (back and sides of the head) reflect the numbers of hairs per square inch the patient was probably born with. By comparing the donor area with other areas that might be balding, we will have very relevant numbers that will reflect the eventual balding that the naked eye will pick up as the balding progresses.
As an exercise in thinking out the process that the skilled doctor performs, follow the thinking on the following case example: Miniaturization in the recipient area (front, top and crown) can often delineate which areas of the scalp are most likely to bald and which are stable, anticipating the patient’s future Norwood hair loss classification. If a 38 year old man has most of the miniaturization in front and very little in the mid-scalp and none in the crown, then the physician may safely assume that the eventual hair loss pattern will probably not go much beyond a Class 3A or 4A pattern (worst case scenario). View the diagram below and click the button for a view of the degree of miniaturization of the patient illustrated here. From this, a Master Plan can be derived depending upon how the existing hair loss is bothering the patient. If the hair loss is just showing some thinning, it may be logical to treat it with finasteride alone, while if the hair loss is more advanced, looks like it is balding and it bothers the patient, then it could be treated with a hair transplant. Because the doctor knows the miniaturization pattern and the age of the patient, he may confidently predict this patient’s worst case and with that information, the patient can budget his time and money to do or not to do a hair transplant. That is why I say that the future management of hair loss needs a Master Plan. In Patient QQ, this is just what happened. He had one hair transplant procedure 10 years ago and because he had limited miniaturization to the frontal area, I could predict that he would probably not need further work for some time. If his situation was to evolve differently (such that he lost more hair than I had predicted) then he could always have had another transplant (if he needed and/or wanted it). He was close to 50 when he came to see me, near the end of his hair loss process. Now his experience with me is just a fond memory of a difficult time in his distant past.
We feel that predicting the short-term loss (the extent of miniaturization in the recipient area, as well as the rapidity of the loss) is critical in establishing the guidelines for treatment, whether it is a hair transplant or drug intervention. In the very early stages of hair loss (the man in his early-mid twenties), findings of increased miniaturization can anticipate future balding even before any loss can be seen to the naked eye. Often, the reason a person seeks a consultation from a hair restoration expert is that there is some change in the “rate” of his hair loss (often more hair seen on the pillow or in the shower). A patient who is very gradually losing his hair is less likely to seek help, compared to a patient who suddenly has acceleration in the rate that he is losing hair. Usually large numbers of hairs undergo miniaturization before any are actually lost and the time the drugs are most effective is in this early phase. In men, DHT is the hormone responsible for these changes.
Ideally, if you are balding, you should take finasteride after mapping your scalp to identify if you have male pattern baldness. The focus upon mapping for miniaturization is to (1) estimate the pattern of hair loss, and (2) measure the starting point for miniaturization so that changes caused by finasteride can be measured over time. Although it takes around 6 to 8 months before you can see the effect of finasteride visually from hair length, it is highly possible that the impact of finasteride on the emerging hair will be earlier than the projected 6-8 months. The measurements are very fast and easy to get from a hair transplant physician and it is today’s Standard of Care that should be available to every balding patient wanting a Master Plan for their future hair loss and hair loss management (medical or surgical).
With successful medical (drug) treatments like finasteride, the miniaturization may be reversed (partly or completely). The responsiveness of each patient is different, so each patient must be diligent in acquiring follow up measurements of the degree of miniaturization and the location of the miniaturization by scalp location. The same diagnostic criteria should and must be followed in women. Without good, reproducible measurements for miniaturization, there is no clinical science in the treatment of hair loss, just hocus-pocus and blustering, a problem that is far too frequent today.
Click each zone or area in the image below to see a microscopic view of the miniaturization (or lack thereof) in a typical balding male:
PZ = Permanent Zone
T1, T2 = Temples
F1, F2 = Frontal
M = Middle
V = Vertex
The below image is a guide to see examples of normal, moderately miniaturized, and advanced miniaturized hair. Click to enlarge.

 “Restoration Robotics, Inc. (Mountain View, CA) is a company using image-guided robotic technology to perform hair restoration by emulating the FUE technique. The robotic technology is in development. Currently, it is not approved by the FDA and the technology is not for sale”, said a company spokesperson when I contacted them. I also found this press release about Restoration Robotics from 2003, here.
“Restoration Robotics, Inc. (Mountain View, CA) is a company using image-guided robotic technology to perform hair restoration by emulating the FUE technique. The robotic technology is in development. Currently, it is not approved by the FDA and the technology is not for sale”, said a company spokesperson when I contacted them. I also found this press release about Restoration Robotics from 2003, here.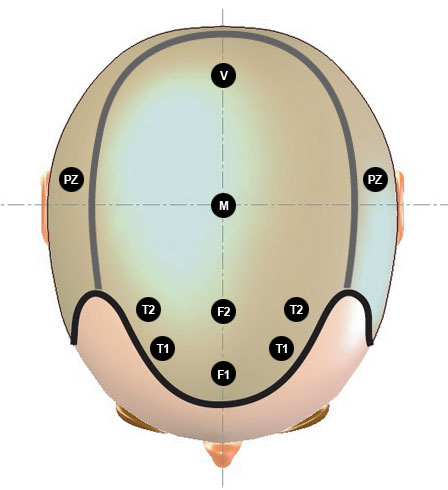


 Great question! Like any good baseball team, you need to have the team work together to get a winning result. What I have consistently said is that a great hair transplant doctor can not produce great work without a great team. In 1991, the quality of the work performed by the hair transplant industry was not acceptable to me, so I had to redesign the surgical techniques to make them acceptable. I have published a massive amount of work defining the standards in hair transplantation techniques (see:
Great question! Like any good baseball team, you need to have the team work together to get a winning result. What I have consistently said is that a great hair transplant doctor can not produce great work without a great team. In 1991, the quality of the work performed by the hair transplant industry was not acceptable to me, so I had to redesign the surgical techniques to make them acceptable. I have published a massive amount of work defining the standards in hair transplantation techniques (see: