![]()
The Pros and Cons for FUE / Strip Harvesting
I’ve put together a nice list of things to consider if you’re interested in having a hair transplant, particularly when comparing the Follicular Unit Extraction (FUE) technique and the Follicular Unit Transplant (FUT / strip) technique.
FUE pros
- There will not be a detectable scar in donor area. Of course the scar will be present after every skin incision, but since scars are very small and scattered in a larger area, they are not detectable even on a head with a close crew cut.
- There are no sutures or staples to be removed. The small pointy wounds on the back of the head will be left to be closed on their own with no sutures or bandages.
- There is minimal or no pain in donor area after the removing the grafts.
FUE cons
- Not everyone is a good candidate for this procedure. We always test our patients before doing the actual procedure with several biopsies with different methods and view the grafts under microscope to see whether we can harvest them without damaging the hair follicles. If we see a lot of transected (damaged) follicles, we can not proceed with this procedure.
- It is more expensive (almost double the cost compared to the strip procedure). Follicular Unit Extraction is very tedious and every graft should be individually extracted by the surgeon as opposed to the strip method where skin is removed first and grafts are harvested under a microscope.
- It takes more time, sometimes up to twice the time when compared to a strip procedure for the same number of grafts. A procedure to harvest one thousand grafts may take six to eight hours.
- A large area of the scalp needs to be shaved or clipped very short. This is not acceptable for many patients.
There are a few issues that are important to look at and understand. Hairs within a graft can be killed by improper harvesting (e.g. drying, cutting it at a critical point in the anatomy of the hair follicle within a follicular unit). This can happen if there is poor cutting techniques in strip harvesting, or in actual transection of hairs within a follicular unit during an FUE procedure. I personally do not believe most of the doctors who claim 95+% successful hair counts from FUE and I would love to pay a visit to some of these doctors and actually do the hair count from their FUE extracted grafts.
Thick grafts (those that are transplanted with fat around the follicular unit) can tolerate air exposure longer than a skinny graft (which can dry in seconds when exposed to the air). But tolerating air exposure for longer than 10-20 seconds suggests to me that hair follicle death may occur and the staff do not have strict quality control process implemented. What is important is not how many hairs are extracted successfully and anatomically intact. The important question to ask is, “Will they grow?”
The best part about strip harvesting is that there is a very high yield with the experienced team. The risks of scar formation that is detectable (greater than 3mm wide) is about 5% with the first procedure, 10% with a second procedure, and higher with a third procedure. Other than the scar possibilities and a slightly more painful recover period of a day or two, the strip procedure is more cost effective and more efficient from a time and yield point of view.
The Propecia and Rogaine One-Two Punch
Do you think the combination of both Propecia and Rogaine is the best one two punch to combat MPB. Do you have any other recommendations as I sometimes get a bad reaction to Rogaine.
I wish it was as simple as that. Some doctors believe that Rogaine (minoxidil) and Propecia (finasteride) together is a good idea and may even provide a synergistic effect. Practicality, however, plays a part and if you consider the finances and twice a day application, it is difficult to use both drugs. My recommendation is to use something that you can be consistent with and stick to it. If you have a bad reaction to Rogaine, ask yourself if it is worth taking it at all.
2007-03-29 11:31:102007-03-29 11:31:20The Propecia and Rogaine One-Two Punch
The Problem of Popping
I would very much apreciate it if you could explain what “Popping” is all about. As I understand it, it limits the amount of hair that can be successfully transplanted.
Popping is a technical term referring to a problem with placing grafts into the recipient sites in the balding area in a hair transplant. The grafts are placed and then do not stay in place, ‘popping’ out of the site. In the early days when we didn’t trim the grafts as closely and the recipient sites were larger, the bulk of the graft was so large relative to the surrounding tissue, that the graft would not be held in place. When the surgeon placed another graft next to the one that was only a couple of millimeters away, the ‘mass’ from the graft into this next site, pushed the last graft that was placed out of the wound. You can imagine a cascade effect, you place one graft and then another and the first pops out. Then you finally get both the first and second secured and place a third when the first two then pop out. That was the way it used to be.
Today things have changed. When we introduced the microscope in 1994, it was evident that smaller and more accurate dissection meant better results than dissection with other less powerful magnification tools. The grafts are smaller and can be more carefully dissected, so that the bulk of today’s follicular units is less than the old minigraft. The recipient sites are much smaller today, we use needles in the 0.8 – 1.0 mm range to make the sites. The results of the smaller site is that the ‘hole’ that is made tends to ‘hug’ the graft and the ‘bulk’ of the graft is of less consequence in the hands of an expert graft placer. Today the best surgeons have staff whose skills have built over years, allowing the grafts to be placed without disturbing the last graft placed. So, popping which was a major problem when we were getting the number of grafts from 500 up to 2000 in 1993, became less of a problem as we moved into the 3000-4000 grafts per session size.
To conclude, your question of popping is more of a historical question than a problem today. What is still relevant today, however, is that surgeons who use larger sites (greater than 1.2mm in size) to manage their grafts, are still practicing older techniques and popping (which is not a problem for us) still remains one for those less skilled in the art of today’s techniques.
The problem of a hair system when you are on a date? (from Reddit)
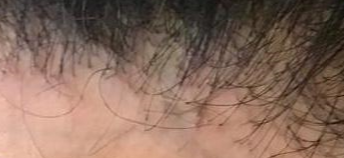
The patient has an absence of vellus hairs from the hairline
With no vellus hairs seen, this is a clear indication that there is some scalp and hair disease present (Frontal Fibrosing Alopecia, or Lichen planopilaris which typically presents as smooth white patches of scalp hair loss. No hair follicle openings can be seen in the areas of hair loss. At the edges of these patches, there may be scale and redness around each hair follicle. Hairs can be easily pulled out. This condition is a contra-indication for a hair transplant. A scalp biopsy will help make the diagnosis.
The Older You Get, Is The Risk of Hair Loss Lower?
Dear doctor how are you? In terms of demographics, I have read on this site the older you become the more hair loss you see. For example, when somebody hits their 30’s, 30% of the people are bald when somebody hits their 40’s, 40% of the people are bald etc. etc.
Could there also be a reversal of those statistics? For example, once a person hits their 30’s and they are not bald or only have minor thinning, 30% chance that they will not go bald and once in their 40’s, 40% chance they will not go bald etc. etc. I know its really hard to judge because everybody is different, but I just wanted your input and wanted to share it with the rest of the readers.
Thank you for a wonderful website site. Take care.
Most balding occurs in men when they’re in their 20s, especially if they are destined for a more advanced hair loss pattern (Class 5 and higher). I can try to predict your pattern during an office visit by measuring your hair bulk and comparing it throughout the scalp. Early patterns that can not be seen with the naked eye can be measured and followed as you get older.
It is important to make your question personal, as none of us fall in any particular percentile, as it is just a statistical process.
The Odds of Going Bald
Hi, I just turned nineteen and have become concerned about hair loss. The corners of my hairline seem high and an abundance of small hairs have sprung up around the hairline. Are these signs of recession, new hair, or can it be either? No one on either side of my family has ever been bald except my great uncle on my father’s side. What are the odds of me becoming bald?
 There is no way to predict your hair loss completely, that is, until you are older. This site is full of information to educate you and if you are concerned, then take charge of your problem. The hairlines in men generally rise between the ages of 19-29 (see Maturation of a Hairline).
There is no way to predict your hair loss completely, that is, until you are older. This site is full of information to educate you and if you are concerned, then take charge of your problem. The hairlines in men generally rise between the ages of 19-29 (see Maturation of a Hairline).
Overall, 50% of men develop some level of balding by the time that they are 50 years old and only 7% will have the most extreme form of balding, Norwood Class 7 (see image at right).
The New Scam in Hair Transplantation
There was a movie named Network that came out over 30 years ago and contained a great line that became a very memorable quote:
“I’m mad as hell, and I’m not going to take this anymore!”
Well, this line came to mind and I want to tell you, my readership, how mad I am and why. Unfortunately, I can not directly act on what is making me mad, except by speaking my mind through this blog. There is a new scam going on in the hair transplant industry, which plays off uninformed patients who come to visit a doctor for hair restoration surgery and who want to rightfully trust that doctor. The scam is simply to get a young man or woman to trust in the doctor through skilled sales and presentation skills, and then when they make up their mind to have a hair restoration procedure, they get what they would not have expected.
The fee structures in the hair transplant industry is based upon a fee per delivered graft. Usually, the prices run all over the place. I have seen three people in the past week alone who received over 2800 grafts, supposedly in their ‘balding’ area. They get poor densities transplanted into the balding area and many more grafts are placed into normal hair. One of the three patients was sold 3300 grafts at $4/graft, and I calculated that he could have never gotten that many grafts because the density of his donor area and the tightness of his scalp would never have allowed that number. Add to that was that my examination only saw about 400 grafts that grew and I suspect that the patient was swindled. Worse than the financial loss, was that valuable donor hair was lost and damage was inflicted in the recipient areas that were transplanted.
I am certain that this scam is being perpetuated all across the world, as I have seen patients coming to visit me from throughout the United States and Europe. All I am addressing here is the intent to defraud. I am not addressing the second class work performed by doctors who try to deliver first class work.
What can you do to protect yourself? The answer to this question is to do careful research. Read the blog entry Patient’s Guide — How Many Grafts Will I Need?, which teaches you how to determine the number of grafts for a given balding area. When I wrote this piece, I did so to explain the economics of hair distribution to arm those prospective patients with enough information to be well informed about the pending purchase of hair transplant grafts, but now it seems that doctors are reacting to the competitive challenge by dropping the price per graft and raising the numbers, many time a multiple of what is needed. Many times the doctor does not even transplant the numbers he/she commits to (I believe this is less common, because their staffs would see that). If you understand the process of calculating the number of grafts, you will be able to determine for yourself how many transplanted grafts you need, so if you (for example) calculate 1000 graft needed and the doctor recommends 3000 grafts, then you know that the doctor is in for the ‘SCAM’. Never forget (that like any service business, even a doctor’s cosmetic surgery activities) that it is a Buyer Beware business.
There is nothing that I can do except to vent here on my blog. I am appalled at the behavior of this group of scum doctors, for they are not only crooks, but they dishonor the good doctors who are in the hair restoration field. If I come out publicly and identify the doctors who I am certain are involved in this scam, I will be open to legal actions by those involved. The medical board has no power to deal with it, as the decisions on what to do falls outside their domain and the doctors would withdraw into the practice of medicine. The only place where these doctors can get attacked is in the courts on a malpractice action. I can play a role as an expert witness to those that wish to take action and would offer my services to the victims of these crimes and their lawyers.
The Medical Science of Hair Loss
What constitutes a good way to follow genetic balding? So far it seems to be a vague art that varies between doctors, and not something that will give an intelligent person an understanding of what is happening to them.
Miniaturization occurs in men and women who are balding. Miniaturization is the process where a normal thickness hair shaft becomes thinner and thinner over time due to the genetically determined effects of aging and/or androgenic hormones on the terminal (normal) hair follicle. The process of miniaturization is a slow process in genetic balding. Hair shafts may lose 10% of their diameter, then 20%, then 30% and so on. Each degree of increased miniaturization reflects further progression of the genetic balding process. The instruments that measure miniaturization were invented (and patented) by me in the early 1990s and they are in wide spread use today. Socially detectable hair loss is not evident until more than 60% of the hair has been lost and as a result, many men do not seek out expert help until they see some evidence of balding (which they too often deny).
When a doctor views the scalp hair with high magnification, the degree of miniaturization and the location of the miniaturization are both critical to establishing (1) the diagnosis and (2) the rate of the process, which progresses over time. Because miniaturization is a relative measurement at any one time (comparing finer hair to the thickest hair), it takes substantial experience before this measurement can be useful to the individual clinician. In our experience, from examining and following thousands of patients with the Hair Densitometer, we have found that assessing the degree of miniaturization has useful predictive value when evaluating the risks of hair loss and in establishing hair loss patterns. The amount of miniaturization in each section of the scalp tells the physician just how far the balding is progressing or has progressed. In men who show more and more areas of miniaturization over time, the genetic balding can be considered active.
A high degree of miniaturization in the upper portion of the fringe area in a Norwood Class 6 pattern (see below in red) suggests that the donor fringe will lower over time so a person who may be a Class 6 pattern balding pattern may become a Class 7 pattern, reducing the fring around the sides and back to a 3 1/3 inch band. A high degree of miniaturization throughout the donor area indicates that all of the patient’s hair may be unstable for hair transplantation and that he may be at risk to have diffuse unpatterned alopecia with extensive balding, even on the sides and in the back of the head (an area normally not affected by any balding or miniaturization in most men). The unpatterned alopecia is characteristic of women’s genetic balding pattern which is often found all over the head including the back and sides.
Miniaturization in the recipient area (front, top and crown) can often delineate which areas of the scalp are most likely to bald and which are stable, anticipating the patient’s future Norwood hair loss classification. If a man has 90% miniaturization in the crown (back of the head) and only 30% in the mid scalp, the physician may assume that the crown is at a higher risk of earlier hair loss than the mid-scalp, giving him an eventual Class 4 or 5 balding pattern.
We feel that in predicting the short-term loss, the extent of miniaturization in the recipient area, as well as the rapidity of the loss, is critical in establishing the guidelines for treatment, whether it is a hair transplant or drug intervention. In the very early stages of hair loss (the many in his early-mid twenties), increased miniaturization can anticipate future balding even before any loss can be seen to the naked eye. Often the reason a person seeks a consultation for hair restoration expert is that there is some change in the “rate” of his hair loss (often more hair seen on the pillow or in the shower). A patient who is very gradually losing his hair is less likely to seek help than a patient who suddenly has acceleration in the rate that he is losing hair. Usually large numbers of hairs undergo miniaturization before any are actually lost and the time the drugs are most effective is in this early phase. In men, DHT is the hormone responsible for these changes.
For the most reliable prediction of the final hair loss pattern, the patient should be over the age of 25 (above 30 is better) and have some visual evidence that the process has started. A base measurement and subsequent follow up measurements are essential to the proper management of hair loss by any doctor considered to be an expert in the field. By understanding these measurements over time, the doctor will understand just what this all means and better yet, the patient now has a way to follow what is happening to him/her. Many young men worry about following their father’s or mother’s male family balding history and come to the office to find out what their future has in store for them. The microscopic assessment for miniaturization is the best way to determine this.
With successful medical (drug) treatments like Propecia in men, the miniaturization may be reversed (partly or completely). The responsiveness of each patient is different, so each patient must be diligent in follow up measurements of the degree of miniaturization and the location of the miniaturization by scalp location. The same diagnostic criteria should and must be followed in women. Without good measurements for miniaturization, there is no clinical science in the treatment of hair loss, just hocus-pocus and blustering, a problem that is far too frequent today.